
Sudden single-sided hearing loss (SSHL), also known as sudden unilateral sensorineural hearing loss, is defined as a rapid loss of hearing in one ear occurring over a period of 72 hours or less. It is considered a medical emergency that requires prompt evaluation and treatment. This article reviews the epidemiology, pathophysiology, clinical presentation, and management of SSHL.
Epidemiology
The annual incidence of SSHL is estimated to be 5-20 cases per 100,000 persons, though the true incidence may be higher due to cases that resolve spontaneously before medical evaluation. SSHL can affect people of all ages but peaks in the 50-60 year age group. There is no clear gender predilection. The vast majority (>95%) of cases are unilateral.
A recent study by Kay-Rivest et al. (2022) estimated the prevalence of SSD in the United States adult population to be between 0.11% and 0.14%, depending on the definition used. This translates to approximately 271,122 to 345,064 adults. The prevalence was found to be higher in older age groups, with the highest prevalence (0.25%) in individuals aged 60-79 years. Women had a slightly higher prevalence (0.17%) compared to men (0.11%).
The prevalence varies by ethnicity, with the highest rates found in non-Hispanic whites (0.15%) and the lowest in non-Hispanic blacks (0.06%). A large South Korean study by Kim et al. found the mean annual incidence of unilateral SSHL to be 17.76 cases per 100,000 population. They noted a slight female predominance, with a male-to-female ratio of 1:1.35. Most patients were in their 60s at presentation.
Pathophysiology
The exact pathophysiology of SSHL remains unclear in most cases. Proposed mechanisms include:
- Viral infection: Viral labyrinthitis or cochleitis
- Vascular: Microcirculatory disturbances in cochlear blood flow
- Autoimmune: Antibodies against inner ear antigens
- Membrane rupture: Rupture of intracochlear membranes
- Cochlear stress response: Metabolic exhaustion of inner ear tissues
In many cases, the etiology is likely multifactorial. Only about 10% of cases have an identifiable cause after thorough evaluation.
Signs and Symptoms
The hallmark of SSHL is rapid onset of unilateral hearing loss, often noticed upon waking in the morning. Associated symptoms may include:
- Tinnitus (ringing or buzzing in the affected ear)
- Fullness or pressure sensation in the ear
- Vertigo or dizziness (in about 30-40% of cases)
- Difficulty with sound localization (determining where sounds are located)
- Trouble hearing in noisy environments
Patients often describe the hearing loss as a “blocked” or “muffled” sensation in the affected ear. The severity can range from mild to profound. There are several risk factors that may increase the likelihood of developing sudden single-sided hearing loss (SSHL):
- Age: While SSHL can affect people of all ages, the peak incidence appears to be in the 50-60 year age range. The median age at presentation is typically 40-54 years old.
- Cardiovascular risk factors: Conditions like hypertension, diabetes, and hyperlipidemia may increase risk due to potential vascular compromise of the inner ear.
- Viral infections: Upper respiratory infections or other viral illnesses are thought to potentially trigger SSHL in some cases.
- Autoimmune disorders: Conditions affecting the immune system may increase risk.
- Ototoxic medications: Certain medications that can damage the inner ear may precipitate sudden hearing loss.
- Acoustic trauma: Exposure to very loud noises or explosions can cause sudden hearing loss.
- Head trauma: Injuries to the head may lead to SSHL.
- Genetic factors: There may be a hereditary component in some cases, though this is not fully understood.
- Stress: High levels of stress have been associated with increased risk in some studies.
- Previous history of hearing loss: Those with existing hearing impairment may be at higher risk.
- Meniere’s disease: This inner ear disorder can sometimes cause episodes of sudden hearing loss.
- Smoking: Some research suggests smokers may have higher rates of SSHL.
It’s important to note that in many cases of SSHL, no clear cause or risk factor is identified. The condition can occur idiopathically in otherwise healthy individuals. Prompt medical evaluation is important regardless of risk factors, as early treatment may improve outcomes.
Immediate Treatment
SSHL is considered a medical emergency requiring urgent evaluation and treatment. The initial management includes:
- Thorough history and physical examination
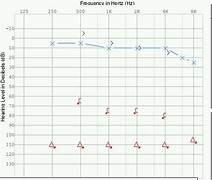
- Audiometric testing to confirm and quantify the hearing loss
- Basic laboratory studies (CBC, metabolic panel)
- Magnetic Resonate Imaging (MRI) with contrast of the internal auditory canals to rule out retrocochlear pathology
The mainstay of immediate treatment is high-dose oral corticosteroids, typically prednisone 1 mg/kg/day for 10-14 days followed by a taper. This should be initiated as soon as possible, ideally within 24 hours of symptom onset. For patients who cannot tolerate oral steroids or present after 24 hours, intratympanic steroid injections may be considered as salvage therapy. This involves injecting dexamethasone directly into the middle ear space. Hyperbaric oxygen therapy has shown some promise as an adjunctive treatment, particularly for severe SSHL or cases resistant to initial steroid therapy.
Long-Term Management
The prognosis for hearing recovery in SSHL is variable. Approximately 32-65% of patients will experience some degree of spontaneous recovery, with better outcomes associated with milder initial hearing loss and earlier treatment initiation. For patients with persistent hearing loss after initial treatment, long-term management options include:
- Hearing aids: For mild to moderate residual hearing loss
- Contralateral routing of signal (CROS) hearing aids: For single-sided deafness
- Bone-anchored hearing devices: Another option for single-sided deafness
- Cochlear implantation: For profound hearing loss with poor speech discrimination
Patients should also receive counseling on communication strategies and environmental modifications to optimize hearing in their daily lives.
Conclusion
Sudden single-sided hearing loss is a relatively uncommon but potentially devastating condition requiring prompt medical attention. While the exact pathophysiology remains unclear in most cases, early initiation of high-dose corticosteroids offers the best chance for hearing recovery. Long-term management focuses on auditory rehabilitation for those with persistent deficits. Ongoing research into novel therapies and regenerative approaches offers hope for improved outcomes in the future.
Stories of People Who Have Experienced Sudden Single Sided Deafness
Stephen Latus: Taking Back My Life After Sudden Hearing Loss
Echoes of Silence: Navigating Life with Single-Sided Deafness
References
- Chandrasekhar SS, et al. Clinical practice guideline: sudden hearing loss (update). Otolaryngol Head Neck Surg. 2019;161(1_suppl):S1-S45.
- Kuhn M, et al. Sudden sensorineural hearing loss: a review of diagnosis, treatment, and prognosis. Trends Amplif. 2011;15(3):91-105.
- Stachler RJ, et al. Clinical practice guideline: sudden hearing loss. Otolaryngol Head Neck Surg. 2012;146(3 Suppl):S1-35.
- Kim SH, et al. Sudden sensorineural hearing loss in children and adolescents: Clinical characteristics and age-related prognosis. Auris Nasus Larynx. 2018;45(3):447-455.
- Rauch SD. Clinical practice. Idiopathic sudden sensorineural hearing loss. N Engl J Med. 2008;359(8):833-40.
- Kay-Rivest, E., Irace, A. L., Golub, J. S., & Svirsky, M. A. (2022). Prevalence of Single-Sided Deafness in the United States. The Laryngoscope, 132(8), 1652–1656. https://doi.org/10.1002/lary.29941
